
Tauzin gave a speech ("THE MIRACLE OF THE MARKETPLACE: HARNESSING ITS POWER – SHARING ITS BENEFITS") at the 2005 Competitive Enterprise Institute Annual Dinner in which he said:
Many countries use a form of "health-care rationing," coupled with price controls. Who, when, why, and how people get to use a drug doesn’t depend on whether they need it – it depends on whether or not the bureaucracy thinks it can afford it. These are policies that put government bureaucrats with a veto right in the examining room with patients and their doctors. Let me give you some examples.
Australians can only obtain a drug that can prevent osteoporosis after they have broken a bone. I guess no one ever told the bureaucrat in charge about an ounce of prevention being worth a pound of cure.
PhRMA often cites scary stories from other countries to make its point that the US has the best system for insuring that new, innovative medicines are available to people who need them to prolong their lives.
As reported in the PharmaGossip Blog, "the Association of the British Pharmaceutical Industry [ABPI; the UK equivalent of PhRMA] has issued a press release and published a manifesto ["The Right Medicine, The Right Patient, The Right Time"] that criticises the lower uptake of new drugs in the UK relative to other selected countries" (see "UK and new drugs: a dog market").
The ABPI press release states:
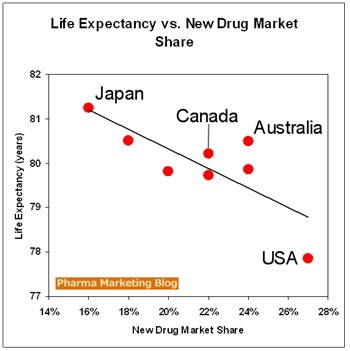
Patients in the UK are still being short-changed by a system that is slow to pick up on new medicines and reluctant to prescribe them even when they have been recommended by NICE [UK equivalent of FDA].To prove its point that the UK is slow to bring new drugs to market, the ABPI provides the following data. For each country the percent of market share of new drugs (those available for less than 5 years) is shown in parentheses:
"The pharmaceutical industry researches, develops and provides medicines that relieve suffering and improve health. We want to make sure that patients receive and benefit from them," said Nigel Brooksby, President of the ABPI.
- USA (27%)
- Spain (24%)
- Australia (24%)
- Canada (22%)
- France (22%)
- Italy (20%)
- Switzerland (18%)
- UK (17%)
- Japan (16%)
As the British Blog Prescribing Advice for GPs points out: "It is unclear if these data are based on items prescribed or drug costs. Additionally, there is no information in this manifesto directly linking the lower use of new drugs to increased morbidity and mortality internationally."
That got me thinking!
 Is there a correlation between the uptake of new drugs and life expectancy, which is a measure of the overall health of a nation?
Is there a correlation between the uptake of new drugs and life expectancy, which is a measure of the overall health of a nation?Just like Billy Tauzin, what I want most from new innovative drugs is to assure I get to live as many years as possible.
So I went to the CIA data site and found the latest stats on life expectancy and plotted that against new drug uptake rates reported by ABPI. I came up with the chart on the left.
Lo and behold! there does seem to be a correlation between these data. Unfortunately, it appears that it is a negative correlation: the higher the uptake of new drugs, the lower the life expectancy!
What can account for this? Billy Tauzin hinted at one possible culprit: "No doubt about it, drugs like these carry potential risk." Billy is asking us to balance benefits and risks "People understand the concept of risk and reward -- otherwise, how do you explain marriage? [whaaaa?!] But that understanding seems to break down when it comes to drugs."
Hmmm... But if the benefits are not there, then I certainly don't understand how to balance benefit and risk.
John
ReplyDeleteYou do realize of course that the statistics you are quoting are completely misleading. We live in America, the greatest country in the world with the greatest healthcare system. Those statistics that you've clearly cherry-picked, actually mean the opposite of what they mean. We live LONGER in the US because our healthcare system is so splendid, and we use more drugs because they are good for the economy, not for long life. We live longer because we are happy.
To paraphrase Orwell:
War is Peace
Slavery is Freedom.
Old age is Youth
Death is life
I don't know if you are being facetious or not!
ReplyDeleteOf course the data are cherry-picked. But the numbers are real -- especially the life expectancy numbers. These come from the CIA, so they must be accurate! I'd go to war on CIA intelligence!
The fact is, Americans don't live longer than a lot of other people. Of course, we do live longer than some.
John,
ReplyDeleteI am stunned that a throw away comment on my site got you working so hard - thanks for this great data!
Of course I'm sure you'll agree that the correlation is not significant and there can be many explanations (other then new drugs) for why the data say what they do but it does raise an interesting topic for discussion.
In response to your other commenter - the data were actually "cherry picked" by the ABPI based on market share of new drugs. John has just filled in some blanks and plotted the data.
Cheers,
Matthew Robinson
Prescriber.org.uk
A more academic look at things is at PMID 15714263
ReplyDeleteMarvellous work from two of my fave bloggers!
ReplyDeleteHurrah for the blogosphere!
PhRMA/ABPI watch out. The truth is coming out........
Why are there 9 countries in the market share table, but only 8 points on the graph? Were you unable to find longevity data for one country?
ReplyDeleteAlso, with the 8 points plotted, if you you remove the USA your correlation disappears. This suggests either a very weak correlation, or that you need more data.
Of course, the data is selective and this is not a scientific study.
ReplyDeleteStill, if all the countries that are listed by ABPI to make ITS point are plotted, including Germany and the UK, there is still a negative correlation. On the other hand, if you remove Japan at the high end and the US at the low end, there is a positive correlation!
What if we had data from very many countries, instead of just a few? The research cited above (PMID 15714263) may have studied a larger database. I only have access to the abstract of that report which states: "We perform an econometric analysis of the effect of new drug launches on longevity, using data from the IMS Health Drug Launches database and the WHO Mortality Database. Under conservative assumptions, our estimates imply that the average annual increase in life expectancy of the entire population resulting from new drug launches is about one week..."
I find that we all select the data we need to prove a point. Take the CommonHealth study I reported on. They decided to report only one slice of their data and then proceeded to issue press releases and get interviewed by leading trade publications. The shame of it was that the publications dutifully reported just the results and conclusions that CommonHealth fed them without any further research.
You might say that my report was similar in that I included the data I needed to make my point, although the same point could have been made with all the ABPI data points, just not as dramatically.
In the end, it's about dialogue, which I am happy to see has happened and, more importantly, comments have served to self-correct one another. This is the benefit of User Generated Content!
Interesting data but I wonder if the average life reflects accidental and other non-drug affected deaths. I would be very interested to see the effect of new drugs against average life expectancy of the subset of the population who dont die in accidents or murder. You cant fairly expect new oncology and cholesterol busting drugs to work on gunshot or car accident victims.
ReplyDeleteOr perhaps it's just that the US year is bigger than everyone else's...
There are many factors that we haven't considered as we look at this issue and one very large one sticks out. If you were to plot the obesity/overweight rates of these countries on the same chart you would find an interesting trend (taken from a quick google search... U.S. 61%, Australia 60.5%, Canada 23%, UK 22%, Japan 20% etc).
ReplyDeleteRegardless of the efficacy of the new pharmaceutical products, we can't overcome the big issue of obesity as it has an impact on every system in our bodies. "Based on researchers' calculations, by the middle of this century the increased risk of diabetes, heart disease and cancer (faced by today's obese youth in particular) could lower the average life expectancy of 77.6 years by as much as five years." ref http://www.mercola.com/2005/apr/2/obesity_rates.htm
Just think of how effective our new products would be if obesity wasn't an issue.