Now that the elections are over, the pharmaceutical industry is left to ponder what the new Congress has in store for it. There has already been a lot of speculation in the general press and trade media (see this
compilation of articles) as well as some shots fired across the bow by Congress.
It's not just democrats itching to get at Pharma. For example, the Senate Committee on Health, Education, Labor, and Pensions (HELP) chaired by Sen. Michael B. Enzi (R-Wyoming), met in full session on November 16, 2006 ("Hearing on Building a 21st Century FDA: Proposals to Improve Drug Safety and Innovation;" access audio and testimony from this hearing
here) and Senator Charles Grassley (R-Iowa) has put a hold on the nomination of Dr. Andrew C. von Eschenbach for commissioner of the FDA (see "
Hold It!").
One bill currently before the HELP Committee is
S. 3807: Enhancing Drug Safety and Innovation Act of 2006: A bill to amend the Public Health Service Act and the Federal Food, Drug, and Cosmetic Act to improve drug safety and oversight, and for other purposes. This bill is also known as the Enzi-Kennedy after the senators that sponsored it. These same senators head up the HELP Committee.
Here's a synopsis of the issues and changes experts have predicted that the drug industry will be subjected to in the next legislative session:
Drug Price Related- Medicare reform -- allow government to directly negotiate prices with pharmaceutical companies
- Allow drug importation from Canada
- Patent Reform -- set limits on whether big pharmaceutical firms can make deals with generic drug makers
Marketing Related- Enact a mandatory 6-month, one- or two-year moratorium on ads for new drugs
- Require FDA pre-clearance of all DTC ads
- Wipe out or limiting tax deductions for advertising expense
- Require a "black triangle" in ads and labels for new drugs
- Set standards for risk presentation that make broadcast ads infeasible
FDA/Drug Approval/Safety Related- Hold up of Prescription Drug User Fee Act (PDUFA) reauthorization
- Make FDA more powerful -- eg, create office of drug safety within FDA, give the FDA the power to fine companies to force them to do safety studies or change the labels of drugs (Grassley-Dodd and Enzi-Kennedy bills)
Recommendations to the Congress by the Institute of Medicine (see "
IOM Report Calls for DTC Moratorium") and the Enzi-Kennedy Bill are top of the list items under consideration as reflected in the testimony before the HELP Committee. See highlights of testimony below. Meanwhile, please consider what your own opinion is:
Take the Pharma Marketing News Online Survey
Pharma Marketing News is currently hosting an online survey to determine how likely these changes are according to pharmaceutical marketing experts. You can take the survey here. You will be able to see a de-identified summary of the current results after you complete the survey. I plan to also write up a summary of the results for the December issue of the newsletter. Your responses are held strictly confidential unless you give me permission to use your name.
Testimony HighlightsSeveral witnesses at the HELP Committee hearing framed the issues and specifically discussed S.3807 and the IOM report. I pick two from "opposite sides of the aisle"; that is, a pharmaceutical company representative and a consumer representative.
Highlights from testimony by Dr. Adrian Thomas, Vice President, Benefit-Risk Management,
Johnson & Johnson Pharmaceutical Group (see
complete statement here).
On S.3807: "We support the use of Risk Evaluation and Mitigation Strategies proposed in S. 3807 to enhance safety, where these strategies are most needed. We believe the proposed Reagan-Udall Institute could be a valuable impetus to spur scientific innovation if consistent and adequate appropriations are provided. We support the provisions of S. 3807 and the IOM report regarding the registration and disclosure of results of confirmatory clinical trials. We support efforts to manage conflicts of interest in FDA Advisory Committees and to enhance transparency while retaining FDA’s access to expertise. Finally, we believe that Congress should adequately fund the Food and Drug Administration in the interest of all Americans."
On DTC Moratorium: "Another remedy that should be reconsidered is the proposed ability of FDA, under the legislation, to impose a moratorium on direct-to-consumer (DTC) advertising for up to two years. This restraint on advertising represents a troubling change. Many members of the industry, including Johnson & Johnson, have voluntarily agreed to exercise restraint with respect to DTC advertising, especially during the period of time after approval. But appropriate DTC advertising plays a valuable role in educating patients about diseases and treatments. The value of this education to patients, as well as the important First Amendment issues that arise from banning truthful speech, even for a period of time, must be carefully considered before legislating in this area. At a minimum, the standard for imposing DTC advertising restraints should be much higher than is currently articulated in the legislation, to ensure appropriate application of this new authority."
Highlights from testimony by Mr. Jim Guest, President & CEO,
Consumers Union (see
complete statement here).
On DTC Moratorium: "In light of the promotional nature of DTC advertising and the long history of abuses in DTC advertising, and given that such advertising strongly influences consumers, Consumers Union recommends a requirement that ALL advertisements be pre-cleared by the FDA for accuracy and honesty, including the growing use of ads in the Internet and other non-traditional sites. In addition, the FDA may impose a two (2) year moratorium on DTC advertising for drugs showing more serious safety concerns. Given the amount of influence this type of advertising has on consumers, and given the potential serious ADRs that may occur years after approval, Consumers Union recommends a moratorium on DTC advertising of three or more years for all new drugs. The history of ADRs and withdrawals shows that drugs cannot be assumed safe after just two years. Adding possible third year to the moratorium authorities in S. 3807 would be prudent and constitutional."
On Off-Label Use of Drugs: "S. 3807 is silent on the issue of off-label use. Given the potential for off-label uses to create serious safety problems, Consumers Union recommends that the FDA develop a program to scientifically study drugs widely used in off-label settings. We are not advocating a ban on such use. We are simply asking that some scientific study be brought to this area, so that the labels on these drugs may be expanded and improved in the cases where the scientific evidence is supportive."
What Do You Think:
Take the Pharma Marketing News online survey.

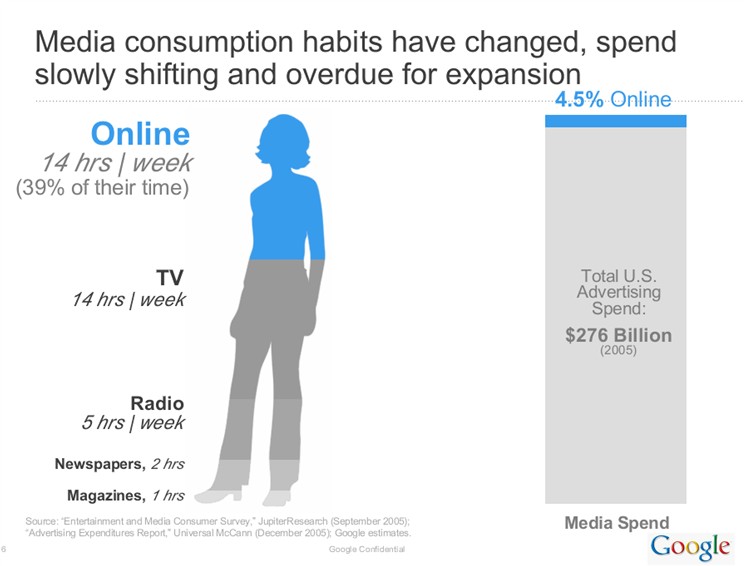 So, it's about time that more attention be paid to the Internet in terms of reaching doctors and consumers where they are spending more time and saving bucks!
So, it's about time that more attention be paid to the Internet in terms of reaching doctors and consumers where they are spending more time and saving bucks!